Making every goodbye count: Bridging the cultural gap in the Intensive Care Unit (ICU)
An article written by A/Prof. Krishnaswamy Sundararajan and A/Prof. Ashwin Subramaniam
This story isn’t unique; however, it reflects how culture and language quietly shape some of the most important moments in the ICU. When my father first arrived in the ICU, everything felt unreal. One moment, he was laughing with us over breakfast, and the next, he was being rushed through double doors, the word "aortic dissection" echoing in my ears like a foreign language. I had lived in Australia for years, but in that moment, English felt slippery and distant, as if it belonged to someone else.
The ICU was bright, cold, and full of sounds I didn’t understand. Machines hummed, and alarms chimed softly. I remember thinking that my father, who loved the warm chaos of our Damascus courtyard, would have hated this sterile quiet.
But the staff met us with a gentleness I didn’t expect.
They noticed small things first.
That my mother clutched her prayer beads.
That my aunt whispered Qur’anic verses under her breath.
That we gathered close, always together, always wanting to be near him.
Instead of telling us to step back or limit our presence, they made space for us. They allowed flexible visiting hours so my mother could sit by his bedside at dawn, when she believed the angels were closest. They dimmed the lights during her prayer. They found a quiet corner for us to spread a small cloth and share food during long nights, because they understood that, in our culture, eating together is how we support one another. Eventually, when he died on maximal therapy, we felt part of the process, and our voice was heard.
The above are excerpts of a consumer’s feedback (anonymised)
When a loved one is in the ICU, and nearing the end of their life, it is one of the most stressful times a family can face. As the case vignette of a real patient illustrates, we all want the same thing: dignity, comfort, and respect for our family members. However, a recent review that pooled evidence from 30 relevant research articles across the globe found that, for families from culturally and linguistically diverse (CALD) backgrounds, this journey is often much harder than it should be. [1]
Why culture and language matter in the ICU
End-of-life care is the holistic support provided when death is near, focusing on the patient’s values and the family’s needs. Unfortunately, people from diverse backgrounds often experience inequitable outcomes, including being less likely to have advance care plans and more likely to receive invasive treatments until the very end, as well as being subject to unwarranted clinical practice variation.
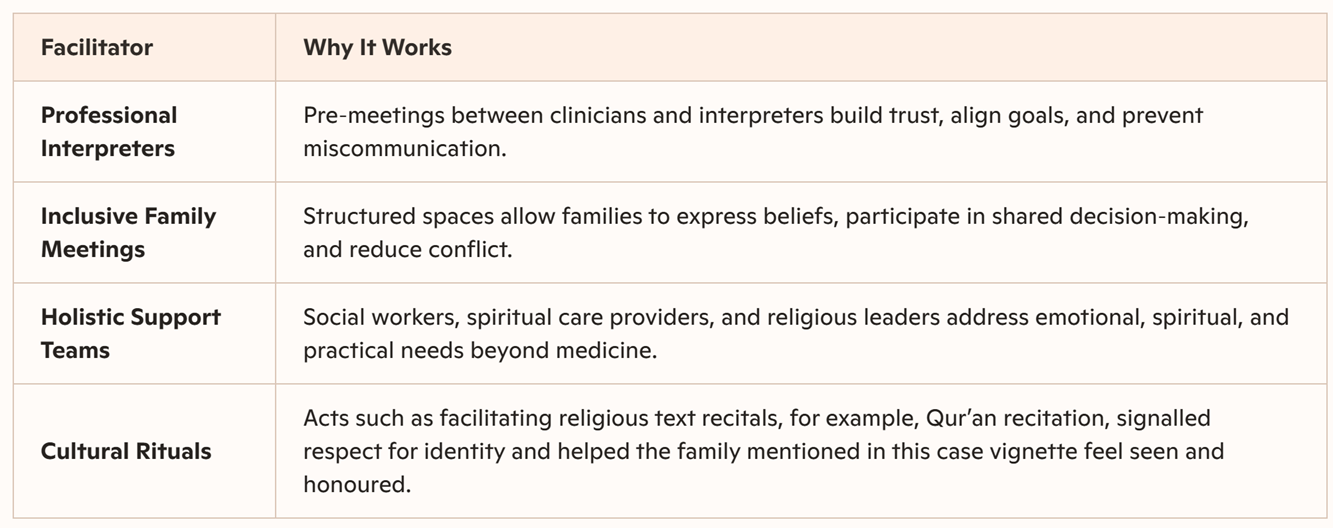
These obstacles often lead to misaligned expectations regarding life-sustaining treatments and reduced access to palliative services. Conversely, the authors identify facilitators of quality care, including structured family meetings, the integration of spiritual leaders, and inclusive bedside practices.
Ultimately, the study advocates comprehensive policy reforms and multidisciplinary collaboration to ensure equitable, person-centred care for diverse populations. These findings serve as a critical resource for improving cross-cultural communication and dignity within intensive care environments.
Why do these gaps exist?
For many families, the biggest barrier is language. Even when professional interpreters are available, they are often underused, leaving relatives to translate complex and emotionally charged information at the bedside. Cultural beliefs can also shape how illness and death are understood...for some families, faith plays a central role in decisions about life-sustaining treatment, which may not always align with medical recommendations. At the same time, clinicians may feel uncertain or unprepared to navigate these conversations across cultures, leading to delayed, rushed, or avoided discussions at critical moments.
Moving forward together
To ensure that everyone receives compassionate care, regardless of language or cultural traditions, our healthcare systems require systemic reform. This includes improving staff training in cross-cultural communication and ensuring that services such as palliative care, which focus on quality of life, are accessible to everyone. When clinicians demonstrate a genuine willingness to listen and learn from a family's history, they build a bridge of trust that makes a difficult time a little easier to bear. In the ICU, booking interpreters early, not at crisis points, inviting spiritual or cultural supports before decisions escalate, and asking families what matters to them before discussing treatments are highly effective interventions, as in the case highlighted. In that setting, where moments are fragile and time is precious, being understood can be just as important as being treated. When systems support clinicians in listening better, everyone - patients, families, and staff - benefits.
Reference
-
Sundararajan K, Aziz S, Anderson N, Damarell RA, Raith E, Phelan C, et al. Insights from critical care clinicians, patients and families from culturally and linguistically diverse backgrounds about end-of-life care in the intensive care unit: A scoping review. BMJ Open. 2025;15(12):e108966.
Authors

Associate Professor Krishnaswamy Sundararajan
Director of Intensive Care
Royal Adelaide Hospital

Associate Professor Ashwin Subramaniam
Director of ICU Research, Dandenong Hospital
Monash Health