

Providing appropriate palliative care in the acute care setting
Related Evidence
- CareSearch – Symptom Management
- CareSearch – Psychosocial complexity
- CareSearch – Prescribing resources
Responding to patients with palliative care needs requires a holistic approach to the physical aspect of symptoms as well as the psychological, social and spiritual dimensions of end-of-life. Clinicians partner with patients, families, and support people, to plan and deliver comprehensive end-of-life care.
From a patient’s perspective ‘best practice is defined more by the qualities and values embedded in the care provided, not a particular program structure or setting’.[1] In addition to symptom management and preparation for death, for patients and families within a hospital setting end of life care that is respectful and compassionate and that maintains a person’s sense of self is important.
Guidance
There are many places that you can find guidance on responding to patient’s needs. Many hospitals already have clinical procedure documents to guide you, but there are also a number of national and state palliative care guidelines that may be more suitable for palliative and end-of-life care.
Assessment
Symptoms
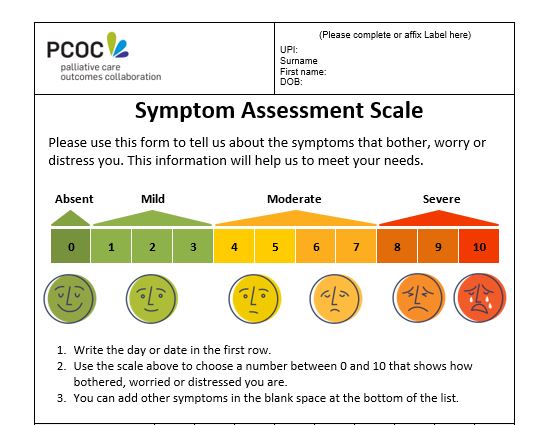
The physical symptoms causing concern can vary depending on phase of illness. Health professionals need to assess and respond appropriately to patient needs. The Palliative Care Outcomes Collaboration (PCOC) Symptom Assessment Scale is a quick and easy way to initially assess patients.
Assessment should also include a check for adverse effects of treatments and whether problems are likely to be due to reversible or irreversible causes.
Distress
Life-limiting illnesses can cause significant distress and suffering for patients and their family. Psychosocial assessment will identify the patients need for psychosocial interventions that can improve clinically relevant health outcomes.
Psycho-existential symptoms are common yet often missed or neglected in palliative care. Screening can be an effective way to recognise and respond to this need. The Psycho-Existential Symptom Assessment Scale (PeSAS) tool can be used to routinely assess patients for distress and suffering in palliative care.
Management
Clinical needs
The CareSearch Nurses Hub has practical advice on responding to a range of physical and psychosocial needs including:
- Symptom management (commonly experienced symptoms – bowel problems, delirium, dyspnoea, fatigue, nausea, pain, skin failure and pressure injuries)
- Medicines management
- Syringe drivers
- Spiritual care
- Family meetings
CareSearch Clinical evidence pages provide summaries of systematic review level evidence for common symptoms seen in caring for palliative care patients:
*note that agitation is dealt with in Advanced Dementia and Care of the Dying Person.
Terminal phase clinical care
For patients in the terminal phase check if your organisation has an end-of-life pathway.
palliAGED has information on Symptom Management when caring for older people who are actively dying.
Responding to psychosocial needs
For many clinicians, guidance on responding to psychological, social, and spiritual needs at the end of life can be particularly helpful. End-of-life Essentials has education on understanding and providing psychological support.
The PalliAGED Improving Care section has practical information for health and care professionals to help with the psychosocial care of older people.
Non-clinical needs
Non-clinical care that supports trust, hope and dignity is important for patients and families. [2] The involvement of trained volunteers to provide companionship can help to relieve pressure from health professionals. Volunteer involvement will depend on the person’s needs and preferences but may include emotional support, reading to them, or listening to their stories.
Interdisciplinary responses
Involving allied health professionals is important. The CareSearch Allied Health Hub outlines how members of a multidisciplinary team can help to meet the broad domains of palliative care needs:
Last updated 29 June 2026