

Providing care at the end of life
Terminal care usually refers to the last few days to weeks of life when a person is irreversibly dying. Management of the last days of life can be supported by discussions that have occurred previously.
Key points
- All medications prescribed at the end of life should be based on careful assessment of the dying person’s condition and symptoms, and doses should be proportionate to the the severity of those symptoms
- Prescribing in end of life care involves a combination of
- Anticipatory prescribing of as needed medications for common symptoms that may occur at some stage when a person is dying and
- Ongoing management of pre-existing symptoms by prescribing regular medications, with additional PRN doses for emergent symptoms
- Medicines that do not contribute to comfort should be ceased. Most patients will no longer be able to take oral medications.
- The subcutaneous route is generally preferred as least invasive and most reliable in dying patients.
- Regularly review symptoms and the effects of treatment. If frequent PRN doses are required or the treatment is for a pre-existing symptom, order a regular subcutaneous dose, and consider using a syringe driver to give the 24 hour requirements and reduce the burden of medication administration. Opioid conversions can be calculated using the EviQ opioid calculator.
- If the patient requires complex medications or has difficult symptom issues, contact the palliative care team for prescribing advice.
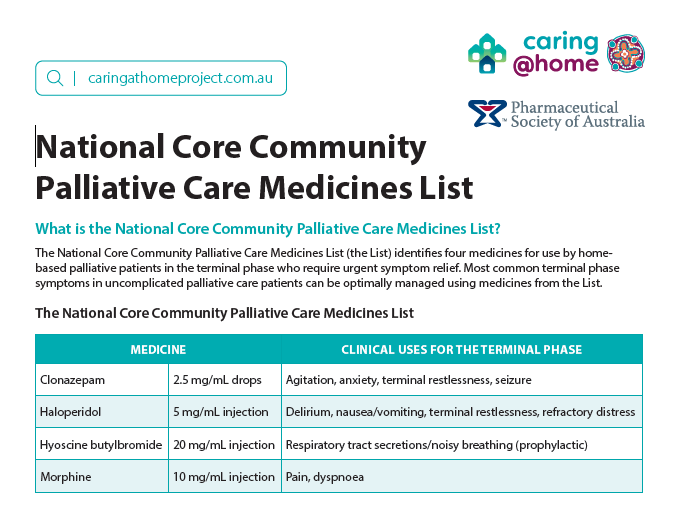
- Sometimes people can deteriorate suddenly. In this case anticipatory medicines may not have been arranged. The caring@home National Core Community Palliative Care Medicines List can guide GPs, nurse practitioners, and other prescribers with their care of their home-based palliative care patients in the terminal phase.
Prescribing information: for managing common end of life symptoms
The following information is based on palliAGED – CareSearchgp app
Key GP resources
Last updated 28 July 2026