


02/07/2026 | Reading Time: 4 mins | Categories: Allied Health / Blog / Community / Evidence / Health Professionals / HP Education / Patients and Carers / Specialist Palliative Care
Telephone-based bereavement support (bereavement telehealth) is a common method of providing care to people after the death of someone close. [1] It improves service accessibility, particularly for those who are unable to access in-person services or have limited internet access. [2] Despite being encouraged by practice standards, [3,4] there is limited guidance as to what bereavement telehealth should comprise or how to provide this important aspect of healthcare. [5] Without best practice guidelines, services fall short of practice standards.
What we did
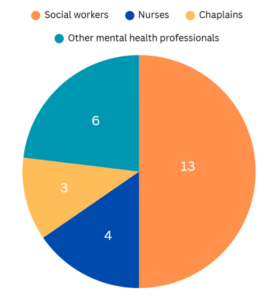
To inform the future development of best practice guidelines for bereavement telehealth, we interviewed 26 bereavement telehealth providers (24 women, 2 men) who worked across a range of settings in Australia, including hospitals, hospices, and palliative care. [6]
What we found
Providers shared their experiences of delivering bereavement telehealth and perceptions of what constitutes best practice. Seven themes were identified:
- A valuable service with limited resources. The telehealth approach can be seen as “less threatening” than in-person counselling and enables “access and convenience” for clients. Bereaved individuals appreciate the service, feeling they could be vulnerable in their grief and “put that ‘mask’ down”. Providers were frustrated, though, by limited resources to provide “routine follow-up” and engage in professional development.
- The first call. The first call is crucial to building trust and connection. Providers focused on being open, using active listening, and allowing for silence and discomfort. They said it was important to convey “empathy and compassion” both “from your tone as well as the words”.
- The dance of rapport. Building rapport was described as a “dance” – developed and maintained over repeated interactions. With trust at the centre of the client-counsellor relationship, providers emphasised “being reliable” and fully attentive: “bereavement calls are important, and they deserve your focused attention”.
- A space to share. Bereavement telehealth offers clients a safe space to share their experiences and process emotions. A core component of support was providing reassurance and validation, for example: “I’m hearing that you’re feeling quite overwhelmed at the moment, and whilst that’s really natural, that must be really hard”. The telehealth mode did make it difficult at times for providers to recognise clients’ emotions, but they overcame this by attending to cues like “breathing and tone of voice”.
- Identifying and responding to risk. Providers emphasised the importance of continually assessing clients’ wellbeing and safety was important, but they often felt ill-equipped to respond to suicide risk. They enquired about risk factors like sleep and social connection and attended to language that might indicate a need for further support. Providers were mindful of pathologising grief by inadvertently interpreting distress as a mental health concern.
- Maintaining contact. Call frequency was decided “on a case-by-case basis” and was flexible to meet clients’ needs and preferences. Some providers also made contact during periods of significance, for example: “I’ll be in contact at typically known, difficult time points; so, that could be beginning of the school year when their child’s name is not on a class list”.
- Training and development. Despite acknowledging the need for a specific skillset to safely and effectively provide bereavement telehealth, providers found it difficult to find accessible and relevant training. They relied on informal and experiential learning and valued self-directed professional development.
Future directions
Our research identified key components of best practice in bereavement telehealth, as identified by experienced providers. However, the efficacy of these practices is still unknown and needs to be tested. Additionally, providers’ capacity to fulfill best practice is limited by three major gaps: 1) Insufficient resourcing, 2) Lack of accessible and appropriate training, and 3) Lack of accessible and appropriate screening tools to identify bereaved people most in need of support and referral. These gaps have the potential to contribute to provider burnout and high levels of stress, ultimately affecting the health and wellbeing of clients. The purpose of bereavement telehealth is compromised by these gaps and must be addressed at funding and policy levels.
Our study is an important step in identifying bereavement telehealth providers’ perspectives of this important part of practice and offers a foundation on which to build evidence-based service delivery that aligns with practice standards.
Key Components of Best Practice in Bereavement Telehealth – Handout
This handout reflects ideal components of best practice as suggested by those in the field, and they acknowledged that chronic resources deficits limited providers’ capacity to achieve each of these.
References
- Kobel C, Morris D, Thompson C, Williams KE. Bereavement support in palliative care: A national survey of Australian services. J Palliat Med. 2019;22(8):933-938 .
- Selman LE, Birchall J, Sutton EJ, et al. Shifting to online and telephone bereavement support provision during the COVID-19 pandemic: A mixed methods study of bereavement service provider perspectives and lessons learnt for current practice. Palliat Med. 2025;0(0)
- Palliative Care Australia. National Palliative Care Standards. https://palliativecare.org.au/national-palliative-care-standards/
- Hudson P, Hall C, Boughey A, Roulston A. Bereavement support standards and bereavement care pathway for quality palliative care. Palliat Support Care. 2018;16(4):375–87.
- Thompson C, Williams K, Masso M, Morris D, Kobel C, Duncan C, et al. Research into services and needs for people experiencing complicated grief: Final report [Internet]. University of Wollongong; 2017 [cited 2026 Feb26].
- Staniland L, Too C, Butshiire L, Skinner S, Breen LJ. Best practice in telephone bereavement support: A thematic analysis of bereavement support providers’ perspectives. Omega (Westport). 2026;92(3):1279-1302.
Author

Dr. Lexy Staniland
Research Fellow
Curtin University's enAble Institute
Tags: Bereavement Care / Bereavement Support / End of life care / Grief Support / Palliative Care Research / Telehealth
136 views
The views and opinions expressed in Palliative Perspectives are those of the authors and are not necessarily supported by CareSearch, Flinders University and/or the Australian Government Department of Health, Disability and Ageing.